This workbook is for my own benefit, when I am experiencing a suicidal crisis and I need help in ways not supplied by other sources (like hotlines). It is based almost solely on my own experience, and not on professional or peer-reviewed sources. I have published it on my personal website on the off-chance it could help someone else with a similar brain who is also seeking help. Due to the topic of the page, frank discussion of suicidal ideation should be expected. I do not describe suicide methods.
For a longer description of my beliefs on suicide, self-help, and community support that influence how I've written the guide, scroll down to the "Why I wrote this" section.
I don't save any information in the text boxes on this page; be aware that refreshing or closing the page may delete your information. If you want to save your answers, copy and paste them somewhere else, or print the webpage as a PDF.
I am still writing this page, and I will be for a while - if you're experiencing a crisis now and want help, seek it immediately, however you are able.
Summary
To-do: I'm probably going to write this at the end
formatting is freaking inconsistent; fix that
First steps: recognition and organizing
1) Slowing down - Is a method of harming or killing yourself close by? Move away from it, or move it away from you. There's no rush; you're about to do a lot of thinking and exercises, and you don't need to put pressure on yourself.
You're probably breathing abnormally. Breathe in, breathe out. Focus your eyes on one thing if you can, or close them. If it helps, make a repetitive calming motion, like rocking. If you're tense, do your best to relax your muscles. Keep doing this until you're ready to move on - however long that takes.
2) What are you feeling? - It is hard to identify emotions, especially when they are strong, complex, and changing quickly. Below are lists of descriptors that may help you figure out what you're feeling - feel free to choose multiple if they apply, or use your own.
My mood is... (terrible, poor, neutral, good, ecstatic)
My body is... (heavy, stiff, light, floating, aching, shaky, tingly)
I have... (pain, nausea, headache, migraine, tension)
I would rate the intensity of my feelings... (a number out of ten)
For how long have I felt this way?
Or, if you're able, type what comes to mind - whether sentences, fragments, or words, having a physical record of what you're feeling is a good step towards being able to articulate your thoughts.
You can be feeling "good" emotions, like ecstatic, happy, and relieved, and still be suicidal. In fact, it is more concerning when I feel a sense of relief, because that means I've accepted suicide as an option. Feeling any emotion (or no emotion) doesn't negate the suicidal feelings, and it doesn't mean you don't deserve help.
Negative feelings like sadness, fear, and anger are necessary feelings, too - sometimes, they're the feelings that just make sense to have. It's better to let them out than to suppress them. Cry, shout, shake, or (safely) throw things - if that is what your body and mind need.
3) Complex thoughts - People usually don't feel suicidal simply because they're a little sad. I get stuck in what I (and others) call loops. These are usually too complicated to be reduced to a single word like "guilt" or "depression". These loops can be:
recent personal life events (a traumatic event, sudden unemployment, the end of a relationship, the death of someone or something close to you, a change in living situation, the birth of a child, a failure or embarrassment)
memories of personal life events (lasting trauma from loss, violence, verbal abuse, rejection, or ignorance; comparing past happiness and success to current unhappiness and failure)
ongoing personal life situations (autism and other neurotype differences, abuse, social rejection and loneliness, identities that don't fit with the dominant culture like ethnicity and queerness, chronic sickness and disabilities, anxiety, mood disorders, financial hardship, a bad living or work environment, underachievement by some metric, boredom)
anniversaries (remembering a family member, friend, or public figure who died on a certain date or age, by suicide or otherwise)
deadlines (telling yourself that if you can't achieve something - feeling better, career success, artistic output - by a certain date, then you will kill yourself)
the idea that you are a burden (emotional, physical, or financial)
the appeal of suicide (as heroism, romance, or punishment for bullies)
general despair (at social, political, economic, or environmental changes or constants)
These are just examples. Write down your specific circumstances, if any, below.
When I don't feel suicidal, I recognize some of my 'reasons' as arbitrary thoughts that only become meaningful when I'm suicidal. For others, I recognize them as real situations I'm in that I can change, or that I can't really help. Either way, my 'reasons' stop being reasons to die. Working on this thought process will be covered in later sections. For now, just write them down.
Maybe none of these examples apply to you. You can have a life that other people consider 'good' - like having people, pets, money, etc. - and still feel suicidal. (Also, 'happy' events like weddings, outings, and successes can coincide with suicidal breakdowns.) The idea that you are 'supposed' to feel good about your life does not negate your suicidal feelings now.
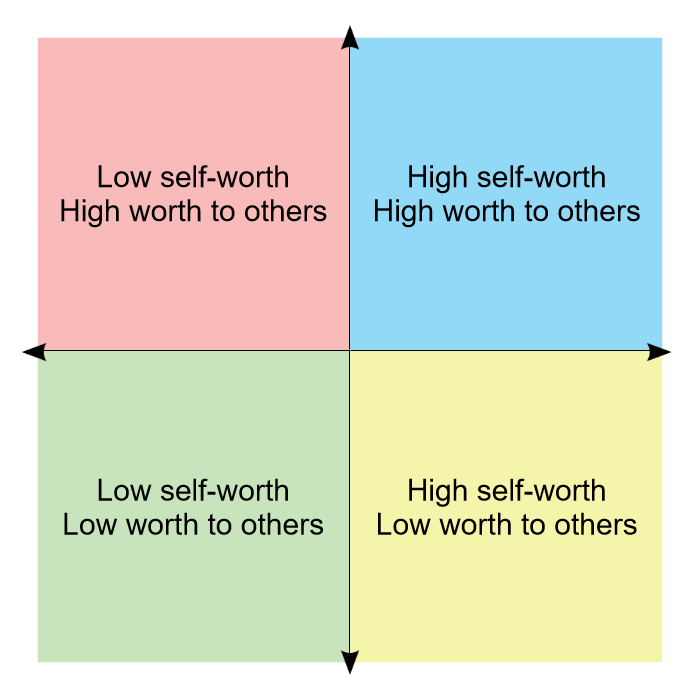
Based on your thoughts and feelings right now, where would you put yourself on this compass?
If you cannot see the compass, think about whether you have high or low self-worth, and whether you think you have high or low worth to others.
This is how you're feeling now - not an accurate description of your permanent self-concept, the thoughts of others, or your place in the world. In this crisis, understand that even things like logic and sense are temporary.
4) Other factors - My suicidal thoughts can be triggered and exacerbated by sensory stress - for example, fluorescent lights, chaotic movement, and painful noises. I think that this is why mindfulness exercises, as they are in mainstream therapy in the United States, don't often work for me - I know what I can perceive in my surroundings; that's part of the problem.
What is going on around you?
I have noticed that I am predisposed to becoming suicidal if I am in physical stress or pain.
Do you need to take your prescription medications?
Are you thirsty or hungry?
Do you need more sleep? do you need less sleep?
Are you aching or sore?
Are you too hot or too cold? Is it too humid?
Short-term, temporary strategies
5) Choosing to seek help - This guide assumes that you are choosing to reject suicide as a solution and seek help. Therefore, the philosophy of suicide, while worth discussion elsewhere, isn't relevant here. This section and the next, "Long-term strategies", can be completed before, during, or after a crisis.
6) "It's not that simple" - Temporary strategies aren't meant to solve your problems. People may have told you to try taking a walk outdoors - this isn't to cure your depressive, anxious, or suicidal thoughts, or fix the situations and events that contribute to you to feel suicidal; it's meant to temporarily alleviate the mental strain, allowing you to pursue more permanent solutions.
First, take care of your bodily functions. Go to the bathroom. Drink some water. Eat something plain. Listen to your body and take advantage of the human instinct to keep going - humans naturally want to sustain themselves and avoid pain.
The following list is a bunch of suggestions that involve no or little social interaction. Not all of them will work for you. You may have been told to do some of these before. You may find it annoying to be told again. But whichever options are within your ability, try them.
Listen to some music - for some people, music of a particular mood works. Think about the emotions you wrote down in the previous section, and whether you want to feel them more or distract yourself from them - both of these needs are okay. Or just put on your playlist of favourites.
Read or watch something - whether it's a novel, comic, TV show, movie, meme; whether it's something new or familiar; and whether it's intellectually stimulating or amazingly stupid, it can help.
Self-stimulate - yes, that sounds rude; interpret as you wish. I like rocking back and forth, swinging my arms, or pressing my skin against something blunt. It makes for a nice distraction. It doesn't quite qualify as exercise, but it does get blood flowing.
Write about it - I make this suggestion cautiously, because for me, writing about suicidal thoughts can make them worse. If you don't think they will for you, write about them - as a description or as fiction. If you're able, you can also write about reasons you don't want to die. The artistic merit doesn't matter; just that they're coming from your head, into words.
Self-care - if it's been a while since you showered, brushed your hair, cleaned your teeth, trimmed your nails, changed your clothes... do those things. If you aren't able, do what you can. Sometimes, I have enough energy to physically brush my teeth, but I can't handle the flavour of the toothpaste. I just brush my teeth with a bit of water. It's not perfect, but it's what I can do; that's the point.
Cleaning - if it's been a while since you cleaned the dishes, wiped the counter, scrubbed the toilet, picked up trash... do those things. If you aren't able, again, do what you can. My living space is perpetually cluttered, and I've learned to be fine with that. But I try to take care of things that are hazards, like dirty dishes and things I could trip on. Even if I only accomplish half of a task in a day, that's still more than it would have been if I had done nothing.
Engage in a hobby - if you like to make art, build computers, play video games, drive remote-control cars, fish... do those things. If you aren't able, remember that "engagement" can mean multiple things. I like making art, but when I'm recovering from a suicidal crisis, I just draw the same things over and over, or I look at art on museum databases online, and I don't worry about creating some masterpiece.
Go outside for a walk - in the neighbourhood, at a park, or anywhere else that is safe and available. If these aren't options, stay inside, but walk around. People suggest this frequently for multiple reasons. Being in a natural area can feel good. Being around people, without the pressure of social interaction, can feel good. Moving your limbs and looking at something else other than your living area can help distract you.
Exercise - if you're able, run somewhere. Lift something. Do squats or pull-ups. Do stretches or yoga. You don't need fancy equipment; my partner uses bags of beans and buckets of water in his home gym.
"Unhealthy" coping mechanisms exist, and while I can't condone them here, there are two things to remember - they may be preferable to being suicidal; and quite a lot of things are fine in moderation.
I've said this a lot, and I will say it more, but do what is within your ability. Maybe you are unable to do any of these suggestions. Maybe you can think of a specific reason, and maybe you can't. Maybe you'd rather just lie in bed until you're asleep. That is okay, too. You don't need to try again until you're ready.
7) Mantras and self-affirmations - among the coping mechanisms, these aren't my personal preference; but I figured I'd include them as a topic here in case people find them helpful.
Mantras (in the sense we English-speakers use outside of religious contexts) can be calming, lighthearted, righteously angry, or anything, as long as they're helpful. Since I don't have experience with them, I don't have any examples. I'm sure plenty can be found online.
You can also try visualizations. None have worked (or even been slightly comprehensible) for me, but again, you can check online.
8) Making a plan - not that type of plan! Just like people make plans in case of a fire or other emergency, it's good to have a plan for suicidal crises. These plans consist of practical and emotional short-term strategies, some or all of which will be available in an emergency.
First, gather the information and items below. Type the information on your phone, or write it on a piece of scrap paper, in a notebook... whichever is usually accessible to you. Then make a few copies and spread them around - in your bedroom, living area, car, or trusted friend's house.
A list of safe places - home, a public area you know well, a safe secluded area... with no severe sensory issues or opportunities to harm yourself.
A list of coping mechanisms, like the ones I listed above, that have worked for you before.
Pictures of people, animals, places, or anything else important to you.
Messages from partners, family, friends, strangers, public figures - whomever you have, saying they love you, care about you, and believe in you. Quotes from media you find meaningful are good too. I keep these on my computer, and I have them backed up on the cloud. At times, I have written them down and scattered them in my living area. I still come across them sometimes.
Emergency contacts - these include anyone you know personally who lives nearby and can respond in an emergency (see the previous item; or neighbour, religious leader...), the police, a doctor, or a local crisis organization. Try to include as many as you can.
The addresses and directions to a local hospital, urgent psychiatric care, or other trusted medical authority.
A "calming kit" with headphones, squish toys, game consoles, childhood toys, a change of clothes, a perfume or oil, water, and non-perishable snacks.
The purpose of this emergency kit is for it to be easily accessible to you when you need it. All of these represent memories and needs that are easy to forget in a crisis.
Next, think of and practice some energy- and ability-appropriate strategies to use in a crisis. If you like to walk down your street in healthier times, practice that - that way, it'll feel more calming in a crisis. If you have a comfort meal, have the ingredients nearby. (Mine is instant ramen and frozen veg. You can buy the noodle cakes by themselves for cheap from an Asian grocery, by the way.) You can use any of the other suggestions I listed above, or any strategies of your own. The point of this step is to establish something you like doing, and make it easier and more familiar. Your mind and body are able to repeat themselves, and repetition is comforting.
Besides setting your next crisis up to be manageable, it is good to eliminate the opportunities you'd have nearby to harm yourself. If it's inconvenient to harm or kill yourself, you're less likely to do that - and more likely to make use of your emergency kit. If you have any weapons, secure them, leave them with someone you trust, or get rid of them (by which I mean sell them, don't throw them in a river). My plans involve substances, so instead of keeping them together in a convenient place, I scatter them in different places - two closets and a cabinet - and I bury them under boxes.
Long-term strategies
9) Making suicide less logical - I've mostly seen suicidal crises depicted as bursts of emotion. Not all of my crises are like that; sometimes, suicide feels the clearest, most rational solution to what I'm experiencing. The short-term strategies above are meant to help with temporary emotions, but they do little to nothing to "de-legitimize" suicide.
To reduce suicidality in the long-term, you have to understand where the suicidal feelings come from, and why they're persistent. You've written about where yours come from in the 'Complex thoughts' section above - at least, for that particular crisis. As for why suicidal thoughts are persistent: they're a biochemical process, and like any habit, constant reiteration makes them stronger. They may come from a genetic predisposition or an environmental response; often (but not always) it's a combination. Regardless, suicidal thoughts seem to predispose people to further suicidal thoughts. Therefore, you'll need to slow or stop that thought process, and replace it with others.
Next comes the process of taking all of the reasons and thought habits you've built up, and dismantling them. I can't write a detailed guide to this process, because it will be different for everyone. I will include some general points of interest and my specific examples of thought patterns below.
I notice several themes in my suicidal ideation:
I tend to think in terms of black-and-white, always-or-never, and all-or-nothing. For example, if I cannot accomplish something to a standard I consider acceptable, I often do not even attempt that task. Or I imagine the people in my life as all-good, or all-bad - their motives, their words, or their roles as influences on me.
I tend to think of the world around me as inherently separate from my existence. I think of myself as unimportant to the functioning of the broader world.
I sometimes think of the world as inherently hostile. I don't think I will be accepted as I am. I think I must conform and hide myself to exist.
I can think in both individualist and communal terms, and I see benefits and flaws in each. I can be deeply uncomfortable with both loneliness and togetherness.
I tend to remember negative experiences in greater number, and with more emotion, than neutral and positive experiences. Sometimes, after a positive experience happens, I later think of it as negative.
I prize logic, rationality, and observation of the real world. Sometimes, I think I am being objective when I am not.
Paradoxically, it feels comforting in some ways to feel suicidal and to give up.
I also ask myself several questions:
How do I think about life? the worth of my life?
What do I take as evidence for the assertions and judgements I make? Am I picking and choosing evidence to fit a hypothesis?
What triggers suicidal thoughts, and do those triggers warrant such an extreme reaction?
To whom and what am I important, impactful, crucial?
One thing I notice is that, at least in the English language, we refer to many aspects of our relationships to ourselves and others in financial language. For example, I question whether my life is worth anything. I wonder how much I and others have invested in me. I wonder if anyone values me. I wonder if the desire to continue with my life is based in a sunk cost fallacy. This is an extended metaphor that I use to criticise myself and delegitimize my inherent right to life. (It is also literal; I think about the quantifiable monetary and energetic costs, and any quantifiable benefits, to keeping me alive.)
Like any metaphor, the one between someone's life and, say, a stock in a tech company is flawed. A life is not worth a particular number; a life is important because of what it is and what it does. There are plenty of ways of looking at the question of suicidality and the importance of life that dive pretty deep into philosophy. I find extended discussions of philosophy dull, so I'll keep this quick.
A religious explanation is probably the easiest to describe, but the least satisfying to an agnostic like me. Religions tend to be against suicide becase suicide is a sin. Religions can also be against suicide because life is an inherent good (good for its own sake), and suicide is the ending of a life. Secular "life is an inherent good" beliefs exist, too, often claiming that the prolonging of life is a natural law.
∞
Another argument that is intuitive to some but not all is that death is frightening. I find that I am habituated enough to the idea of death that I do not find it as frightening as others do, so this is not a good argument by itself for me.
Self-harm and suicide are painful (physically or emotionally) and hard to carry out. It's hard to die, and failed attempts can cause more personal suffering and irreversible problems. This is a pretty convincing argument for me.
I often see suicidality described as a lack - of hope, meaning, purpose, freedom, occupation, or foresight. One or all of these lacks may fit your crisis. This frames suicide as a fixable problem. I don't prefer this argument alone, since improving these circumstances - getting "better" in simple, observable ways - does not necessarily make the suicidal ideation go away, nor fix any other problems you have.
∞
One of the most common phrases in my ideations is the idea that I am a burden or inconvenience to others. This is one of the most insidious ideas, because it seems very easy to prove. I've felt suicidal looking at my monthly expenses, firstly because I was wondering how I'd keep paying them, but also because the huge numbers just felt like a waste on someone like me. I don't think it's a coincidence that many suicidal people consider themselves a financial burden, given the flawed metaphor between financial worth and the importance of life that I identified a few paragraphs above.
I've also felt especially guilty and depressed thinking about "emotional investment" - again, thinking about it as currency. I've thought about the people who do chores for me when I'm too overwhelmed, or to whom I talk about the overwhelming things in my life, and I wonder if they, too, see it as wasted time and effort. In reality, that isn't how love works. Love and care aren't things to trade, tally, and tax; they're ineffable concepts by which close human bonds form. Love makes it easy to care for the person you love. These people are caring for you because they want to. I'm still trying to convince myself of this.
If you're insistent on looking at your life from a utilitarian perspective, you can use a hedonistic calculator - a method of thinking that, put very simply, compares the hedonistic (pleasure-giving) benefits and drawbacks of your suicide versus your continued natural life. For example, your suicide may cause extreme and prolonged grief among the people to whom you are important, which is bad, and would not happen if you keep living. You could even extend it to include the trauma and inconvenience of people to whom you aren't as important, but who would still be impacted by your suicide. As another example, your suicide will remove the potential for any positive impact your life can have on the world, like the ways you would help people in the future. This way of thinking, by itself, is not always helpful to me in a suicidal crisis, because I forget that I have close connections whom I would upset. And some people may genuinely have few close connections. Not everyone has supportive people in ther lives. I still believe these people have a right to exist, so I don't use this way of thinking by itself.
∞
More common arguments against suicide are that suicide removes your ability to make choices and enjoy life. Suicide is permanent - since death is permanent - and the non-existence of the person after suicide means they cannot have liberty or happiness, considered by many to be inherently good things. Put in simpler terms, if your suicide does not happen, you will continue to live, you may have fun, and you may be glad you didn't do it later on. You may even become a motivational speaker. This way of thinking is sometimes helpful to me, but sometimes not, especially because thinking about the future in neutral or optimistic terms is difficult for me in a crisis - I cannot imagine my life becoming better in these moments.
Yet another common argument is that suicide is impulsive and irrational. Many people seem to act on impulse, due to strong emotions and the availability of a method. These states of being are temporary; and people who survive the act may later wonder what they were thinking and why they wanted to die. Suicide can also be seen as a disproportionate response to anything a human can do or experience. Usually, this argument takes the form of the phrase, "[something] is not worth killing yourself over". This thinking helps in a few of my crises. But if I had been through severe trauma, I'd find it very condescending.
∞
Related to the previous points is that many object to the idea that suicide is a choice that just anyone should be allowed to make. This view sees many examples of suicidal ideation as an affliction - a symptom of a disorder that requires treatment. This disorder may interfere with the suicidal individual's ability to see other perspectives and make rational decisions. As an example, someone with depression has depression, which is a disorder of the mind not inherent to the individual's identity; it is the responsibility of a medical professional to treat, and it would benefit the individual if it were gone. But because of the individual's depression, they see suicide as an option. They are not thinking rationally when they are considering suicide, and they should be discouraged from making that choice - according to this perspective. This is a common perspective of people I know in the medical field, and I do find it helpful in my crises, if imperfect - I'm cautious of anything that interferes with a person's autonomy, and sometimes I feel that my ideation is not closely tied to depression.
∞
Autism is different from disorders like clinical depression - it is not removable from an individual's identity. (Some or all of the following argument can be extrapolated to other types of permanent or long-term disabilities, identities, and states of being. I am using autism as an example, because it is most important to me.) Thinking of myself as having a permanent disability is depressing and scary. But because it explains a lot of the abuse and rejection I've experienced - the same events that come up often in my suicidal ideation loops - it's important to understand how autism, and other permanent aspects of ability and identity, change how I see myself and my place in the world.
An important idea that is the focus of justice movements is that of the human differences in identity and status - like sex, gender, sexuality, age, ethnicity, country of origin, neurotype, health, disability status, socioeconomic status, history of trauma, etc. - none of these take away from someone's right to live. Someone's self-concept, self-worth, and self-confidence may be negatively impacted by perceptions of any of these categories. This destruction of self may be explicit or implicit; and it may come from individuals, groups, or institutions. It is well-studied that certain demographics in certain areas are at higher risk of suicide. Be cautious of anyone saying your identity is "just an excuse" to complain, because that is a reductive approach that ignores evidence and basic empathy. (One of the notable high-risk demographics is female autistic adults with mood disorders.)
It is unfair to die for something that is not your fault. It is unfair for you to feel suicidal for factors outside of your control. To reject suicide as someone in a high-risk category is to recognize that a lot of us aren't meant to succeed, and to choose to direct the disappointment and anger to injustice instead of to ourselves. Under this framework, it is good to keep living, because that is the justified thing to do. It is hard to keep living in a world that says it does not want or need you, but that makes it more important that do the defiant thing, which is to live in spite of that. This argument is so grandiose that it makes me laugh! But I think there's enough truth in it that it helps me a lot in certain crises.
∞
Any of the above arguments may work for you, or they may be unimportant, not applicable, or annoying. They're just the thoughts that have come to my mind. I'm happy to hear more arguments against suicide - you can email me, or use the link for the anonymous form at the bottom of the page.
10) Reaching out - community assistance Many suicidal people, myself included, do not seek help from other people in a crisis. There are plenty of reasons we don't, and plenty of ways to remind ourselves that we need and deserve help.
A suicidal crisis may happen at an odd time, and I think I'll be bothering people if I reach out to them. I don't want to wake people up, interrupt their lunch break, or bring down their holiday. That's why it's important to have several options - if everyone in your time zone is asleep or busy, you can turn to an online support group with members around the world. Or you can call emergency services - it's their job to stay awake to help people like you.
You may have been told that by reaching out, you're seeking attention. Duh. Of course. That isn't a bad thing! If you are in a crisis, and you are reaching out, that is not manipulative. You are asking for help because you need help. It doesn't matter if this is your first time feeling suicidal, or you've felt suicidal your whole life. It doesn't matter if you feel embarrassed, or if you feel like an inconvenience. It doesn't matter if you've attempted suicide before or not. It doesn't matter if you feel acute pain, or just a vague sense of malaise. The people who brush you off are not the right people to talk to about suicidal feelings.
Your requests for help may have been repeatedly dismissed. I was told my depression came from hormones, puberty, and middle school, and that I'd outgrow it (I did not). Being prone to emotional disregulation does not mean your emotions are not legitimate. Feeling emotional does not mean there isn't something wrong with your circumstances, too. It is not for other people to decide what is or is not a legitimate claim to feeling suicidal. Again, if you want help, you should get help.
With all this said, I don't recommend telling just anyone about your suicidal feelings. First, you shouldn't tell people who make you feel unsafe. These include people who abuse their power over you and people you don't trust to respect your privacy.
Besides those people, a lot of people just aren't emotionally equipped to understand and help with suicidal feelings. They may only repeat phrases they've read online that may be unhelpful or even harmful, even if the person means them well. Even people who offer help can find that your crisis is too much for them to handle.
There are also people dealing with their own suicidal thoughts and depression, or other overwhelming circumstances, and they don't have mental capacity to spare for you. If you discover someone like this, do your best to understand and accept that, convey that to them, tell them you care about them, and give them some space.
If someone is to act as a support for you - whether it's just once, or every time you have a crisis - it's good to communicate that, and make sure you have their consent. It's an unpleasant surprise for someone to receive an emotional dump from you that they weren't expecting. If you ask people beforehand, many are willing to help to a limited extent, within their ability.
Rejection doesn't mean that no one cares - it just means that you'll have to find someone else.
11) Seeing a shrink - Professional assistance - There are several types of mental health professionals, and it is not always clear which will be most helpful. Some are generalists, and some are specialists. Often, one professional can only help to a limited extent, and then they refer you to another. Some professionals are embarrassingly uninformed about their fields of expertise. Others are really wonderful and helpful people who can change your life. Most are somewhere in between. You don't know how a professional will be until you try them. In addition, some forms of medical care may be difficult for you to access due to location, scheduling, finances, or disability. The options you have will vary. I recommend using a search tool - for example, on the internet, on a map, or through your insurance.
None of what I've described below constitutes specific medical advice. The purpose of this section is to help you manage expectations and notice red flags.
You may already have a primary care provider; if not, it's usually quick to find one. Primary care providers vary widely, and not all will be a good fit for you. They may or may not know much about conditions like psychiatric disorders or autism. Whether they can prescribe medication depends on the laws in your area. It's good to adjust your expectations based on these limits - but if you have a bad experience with a primary care provider, it is perfectly fine to switch to another.
In an ideal world, psychiatrists are better equipped to handle mental health issues. Some may specialize in child, adolescent, or geriatric patients; if you're an adult, contact the office to check if they'll take an adult patient. Some will offer medication management by itself, and some will require you see one of their therapists, even if you're receiving therapy already. It will be more expensive than just seeing your primary care provider, but it may also be more beneficial.
You may come across a psychologist when seeking an evaluation for something more complex than anxiety and depression, or in treatments like psychotherapy. A psychologist is not able to prescribe medication.
More specialized doctors who study and treat mental health issues include developmental disorder specialists, neurologists, sleep specialists, gynecologists, and endocrinologists. Dieticians and pharmacists, who are registered experts but not necessarily doctors, may also contribute to mental wellness. Whether you'd benefit from any of these is a discussion for yourself and your primary care provider.
There are several types of therapies. These include cognitive behavioural therapy, dialetical behavioural therapy, Gestalt therapy, art therapy, and animal therapy. All of these have proponents and controversies, and one or several may be of use to you. Therapy can be individual or as a group. It can also be neurodivergent- or queer-affirming. Several types of nurses, therapists, counselors, and social workers are qualified to administer these therapies. In all of these therapies, your needs and goals should be prioritized.
I have had positive and negative experiences with several types of professionals. Since everyone has different needs, and since it seems to be a crapshoot whether you'll get someone who fits your situation well, I can't make specific recommendations. However, I can include some red flags I've experienced or heard of.
Some professionals are impatient or dismissive. While it should be understood that professionals have limited time and that there's only so much you can accomplish in an hour, professionals should make an effort to respect your concerns. Indications that they are not doing this include constantly interrupting you, denying your problems, citing very outdated medical knowledge, or ignoring an official diagnosis from a specialist. You should be an active participant in your own medical care, and you should feel able to express concerns. Even if a professional believes you are incorrect, they should be polite and clear, or refer you to someone who is qualified to give you an answer. If the way they treat you is especially egregious, you may want to consider reporting the provider to a medical board.
Some professionals (and their offices) are very disorganized. Several times, I have had to call an office repeatedly to remind them that they were overdue for something they had promised they would take care of. This is especially difficult for someone who is autistic and anxious. Sometimes, the communication was so poor that it could have violated the ethical concept of informed consent - the idea that a patient should understand enough about a potential treatment and its side effects to make a choice on whether they want it.
One professional I saw outright scammed me - I can't put it in less severe terms than that. I told them I wanted medication management only, not therapy, as I was happy with the therapist I was seeing at the time. They scheduled me for weekly $100+ half-hour appointments during which the psychiatrist asked me about what had happened that week. I answered, taking the questions at face value. The psychiatrist told me a few unhelpful things (such as, paraphrased, 'why does verbal abuse make you upset? You should just ignore it.') When the bills came, I realized they were charging me for psychotherapy, on top of (and at nearly twice the rate) of my current therapist, after I had explicitly told them not to. They also refused to consider it a billing error.
Other red flags include HIPPA violations (certain violations of the privacy of your medical information) and abuses of power, whether physical, sexual, or emotional.
Certain people, including the above medical professionals and other people like those who work in schools or in law enforcement, could be mandated reporters of imminent suicidality. (Exactly who is legally a mandated reporter depends on laws in your region.) If they suspect you to be an immediate danger to yourself, they may be legally required to report you to state government medical offices. They may also call emergency responders, who may take you to a hospital for acute psychiatric evaluation and treatment.
This is supposed to be in your best interests; but the overstimulation and uncertainty of this process could be overwhelming for autistic people. And in general, you may worry about the cost of an ambulance or hospital stay, or the loss of autonomy. You may worry that even admitting occasional thoughts of harming or killing yourself will be taken as an immediate threat. As a result of these beliefs, sometimes people who feel suicidal don't disclose that to medical professionals.
The purpose of hospitalization is not incarceration - it's meant to be medical care, not punishment. And in many cases, a professional can differentiate between someone who is experiencing passive suicidal ideation and someone who is going to harm themselves without immediate intervention. Concerns you may have about seeking help make a lot of sense, but ultimately it's best to be honest with a medical professional about what you're thinking.
Medication is one of the most personalized aspects of mental health. What works amazingly for one person is counterproductive for another, for reasons no one quite understands. Medication is not usually a quick fix. It doesn't tend to work perfectly or immediately. A particular type of medication may not work for you at all. You may have to try several before discovering one that works, or finding that medication isn't for you. This can be really devastating to someone who places a lot of hope in medication working.
It is your right to ask about side effects. Various antidepressants have side effects that can make suicidal feelings worse. Ask your medical provider what you can do to prepare for side effects and what to do if they're overwhelming. Make sure you have a scheduled check-in or other plan to make sure you're alright, and record symptoms in detail as you experience them.
The last thing to be aware of is the disconnect between different forms of treatment and care. Your primary care doctor is not usually in constant contact with your therapist and psychiatrist about you, for example. It's up to you to keep all of them updated on the others' actions and your state of mind.
12) Recovering and remembering - When my suicidal crisis ends, for a period of time, I feel empty. Sometimes I just feel a bit strange and unsettled - my reaction to what was once intense suicidal ideation is, "huh, that was weird. I went a bit nuts." In other cases I feel completely unbound from my body. My visual perception is like a distant television, not interactive or important, just background noise. There is no physical or emotional feeling, and sometimes there is no me anymore, just a body with vital signs. I don't have a better way of explaining it except through these strange metaphors.
This second crisis, related to but distinct from the suicidal crisis, subsides over a period of time that ranges from minutes to weeks. After this is over, I can think about the crisis process somewhat objectively - unless, of course, I immediately hit the next crisis.
I realize my memory does not always treat me kindly. My suicidal habit is so strong that it overrides what I know. I'm surprised by what I've selectively recalled in my crisis - the worst of what people have said to me, the most harmful and avoidable mistakes I've made. As I recover from my crisis, I remember things like:
A plan for a solo trip to the park that I made for the weekend
A bag of chocolate chips in the fridge
A leucistic pigeon I saw pecking at a French fry on the sidewalk
An in-progress dispute for a parking ticket (someone had spray-painted the sign; how was I supposed to know?!)
An order for my partner's birthday gift that I have to place
The pounding of my neighbour's Saturday night television
Guo Xi's painting, Early Spring
A snake (Storeria dekayi) from a meme
A kind message from someone who had no reason to send it, except kindness
The fact that "pled" and "pleaded" are both valid past-tense forms of "plead"
I think calling these "beautiful memories" is cheesy, and a bit of a stretch. But I think I am genuinely glad to see them through. Even the damn parking ticket.
) Fairer expectations - on yourself and others. your own abilities and limitations, reducing guilt, self-forgiveness. allowed to make mistakes, even big ones. can feel personal responsibility without "convicting" yourself. My belief is that human's inherent worth/right to live does not come from usefulness. deserving to live
including self-affirmation/external affirmation - validation, not in a cheesy way. Unconscious, internalized stuff from people's comments, perceived opinions (still working that out)
The value of positive thinking - if this paragraph makes you feel annoyed, read the next one, too.
The value of negative thinking - positivity is annoying
The truth in the words - ideations come from somewhere. suicidal feelings come from somewhere. Even if you (like me) choose to view suicidal feelings as irrational and you reject them, there is still useful information to be gained. Read through your loops with a clearer mind; you'll notice patterns... for example, my suicidal feelings are often severe when I have financial anxiety, when I experience autism-related discrimination, and when miscommunications happen between my closest friends and me. - use info, change what you're able. what you can't change - either accept, or get mad about it (some things are worth being angry about; some things are genuinely not your fault)
) Small life changes - being okay with, or working to change, imperfection. Small self-accommodations. 'Content' (social media, warnings)
) Big life changes - external (reaffirming or ending relationships, job, living situation) and internal/personal - coming out (unmasking as ND, queer, etc.) safely, explaining to others the need for change/self-advocacy (and accepting some people aren't going to be convinced)
) Preparing for relapses - suicidal feelings will probably stick around. They may stay, or come and go, for life. what to do
) Reckoning with a nonsensical life
Why I wrote this
I wrote this because what I'm looking for in suicidal crisis relief doesn't exist in a convenient format or at an accessible price. It is written according to what works for me - the personality and beliefs I have, the place I live, and my own abilities and limits.
I have put this workbook on my website because, as I said, I want it to benefit people who are like me, in some or all of those ways.
I also have heard people say, "let's talk about mental health and suicide". But sometimes, public discussions on these topics don't cover necessary issues. Other times, people conflate discussion with dramatization. (I've lived with frequent suicidal thoughts for well over a decade at this point, and most of the time they're more of an annoyance than a tragedy.) And sometimes, public discussion of suicidal people mischaracterizes us as pathetic or dangerous. As a result, can be difficult to find useful discussions about suicide for laypeople.
When reading and using this workbook, it is good to know that it is written by autistic person. I suppose that I am "low support needs", although it sure doesn't feel like it. But I live independently, and have a romantic partner, friends, family, and material resources. This context is important because autistic people with different abilities, disabilities, and support needs will have different communication styles and accomodation needs.
The disability rights movement informs my beliefs - this, according to me, is the idea that being disabled does not take away from your inherent worth as a person and right to life, and that accommodating the disabled to an equitable position in society should be seen as a necessity of justice, not optional or a burden. This legitimizes belief in the necessity of institutional change. I hope that allistic people can make use of this workbook, too.
All this means I have lived experience in what I am writing about. I do not, however, have a degree, and that is important too. I wrote the workbook guided by my own thoughts and experiences, not by peer-reviewed scientific research and data. Both types of evidence are important when trying to understand suicide, and if you are able, I suggest engaging in scientific research and consensus too.
The limitations of this workbook
There are some assumptions and omissions in the workbook based on what I have and have not experienced.
The workbook does not include specific advice for substance abuse disorders, other psychiatric disorders, physical disability, or intellectual disability. I am not qualified to discuss these in detail in any sort of advisory role. I also don't discuss legal recreational drugs; they just aren't for me.
I also avoid any pro-suicide beliefs. I do not attempt any objective justifications for suicide or any of its forms, including assisted suicide. I avoid discussing people who do not want help and who want to die. They are simply not the focus of this workbook. I don't categorically agree or disagree with them; they just aren't my target audience. This is out of necessity for me, because thinking about justifications for suicide make my own ideations worse. For the same reason, I do not describe suicide methods.
Flaws in existing self-help media
Besides avoiding what I am unable to talk about, I also avoided topics that I just find useless or harmful.
I use matter-of-fact language. I avoid what I think of as overdramatic, flowery language. I find that it misrepresents what suicidal ideation can be.
I use literal language. I avoid metaphors and visualizations, which I find confusing.
I avoid a purely emotional concept of suicidal feelings. I've noticed that other sources have a strong emphasis on emotional pain. That is often, but not always, a factor.
I avoid the idea that crises should be dealt with by "thinking positively", "looking on the bright side", and "focusing on the good". I think this pathologizes negative thoughts like sadness and anger that are sometimes the most appropriate response to a situation, especially when that situation is traumatic. I also think it's difficult for anyone, especially autistic people, who often struggle with emotional identification and regulation, to just "feel better" on command. Negative feelings don't just go away when they're covered up by positive thoughts - it seems to be better in the long term to process the negative emotions.
I avoid the "everything happens for a reason" narrative. I find it really condescending and unhelpful when circumstances are out of my control.
I try to minimize "cure", "it's bound to get better", and "total recovery" narratives. These false promises suggest that suicidal feelings are like a mild virus you eventually get over with some medication, and not a chronic condition that could require long-term or lifelong monitoring and management. What suicidal feelings are, and whether they will relapse after treatment, will depend on the individual and their circumstances.
I try to avoid what I call the "self-help grind". This idea puts the responsibility of having suicidal thoughts, and recovery from them, solely on the suicidal individual, which I don't think is fair. It also makes feeling suicidal sound like a conscious choice, and not a result of medical and environmental factors.
I completely avoid the argument that "other people have it worse" or that suicide is "selfish". I see this so much, and I hate it! If you are feeling distressed about feeling suicidal, you are feeling bad, and your feelings are important. You should not be shamed for feeling suicidal. Everyone's worst day may be different, but that doesn't take away the fact that worst days can be really devastating for anyone. I also hate the idea of putting other people down to feel better about yourself.
I avoid promoting the idea that "suicide attempts are cries for help" or "attention-seeking behaviour". It inaccurately reduces a suicidal person's experience to one motive, and it's an excuse for not respecting, understanding, and providing care. People who attempt suicide require medical and community attention; they do not need to be accused of faking.
I avoid religious arguments against suicide - since I am not religious, they are arbitrary to me. The same goes for arguments that suicidal ideation and action are morally wrong. My workbook (and general philosophy) on suicide is informed by, but not strictly adhering to, Absurdism - which I interpret to be the belief that there is no objective meaning of life, but that people's search for a meaning of life makes living worth the trouble. This accomodates individual religious and moral beliefs without claiming everyone needs to follow a specific religion or morality.
I avoid heavy philosophical discussion of suicide, because I think it is boring. No other reason!
I have made an anonymous workbook feedback form if you would like to provide anonymous feedback and comments. I cannot respond to this form.
If you are okay with being identified, and you'd like a response from me, but you'd still like to provide feedback and comments, you can send an email (the link is at the bottom of this page).
Personal accounts, venting, and descriptions of suicide attempts will not be responded to right away. This is because I need to control when/how I engage with this topic, for my own health.
Any harassment or threats will be ignored or reported.
This workbook has come about thanks to the support - practical and emotional - of several people close to me. Without exaggeration, I owe them my life.